Even when motivation is the same, access isn’t. This study shows that Medicaid patients can achieve comparable outcomes—if given the same tools.
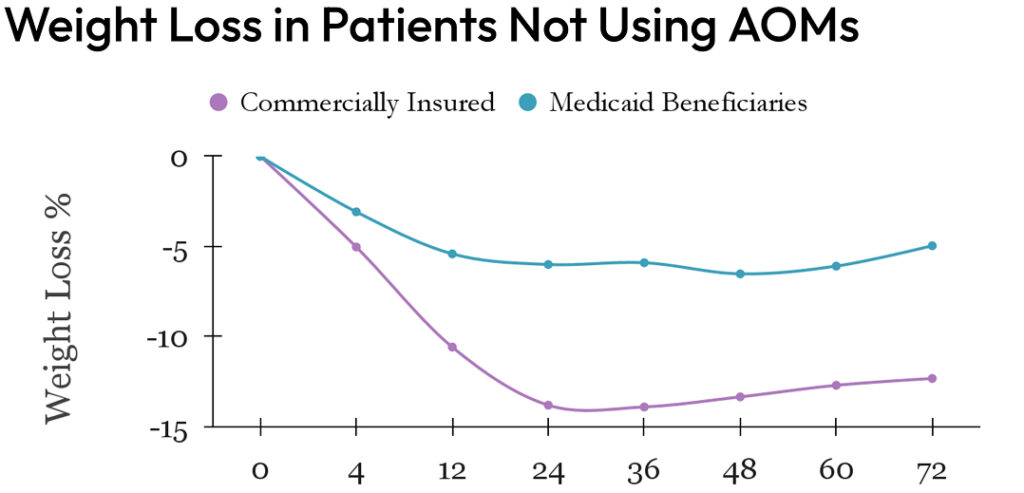
Without AOMs: Medicaid patients lost 5–7% less weight
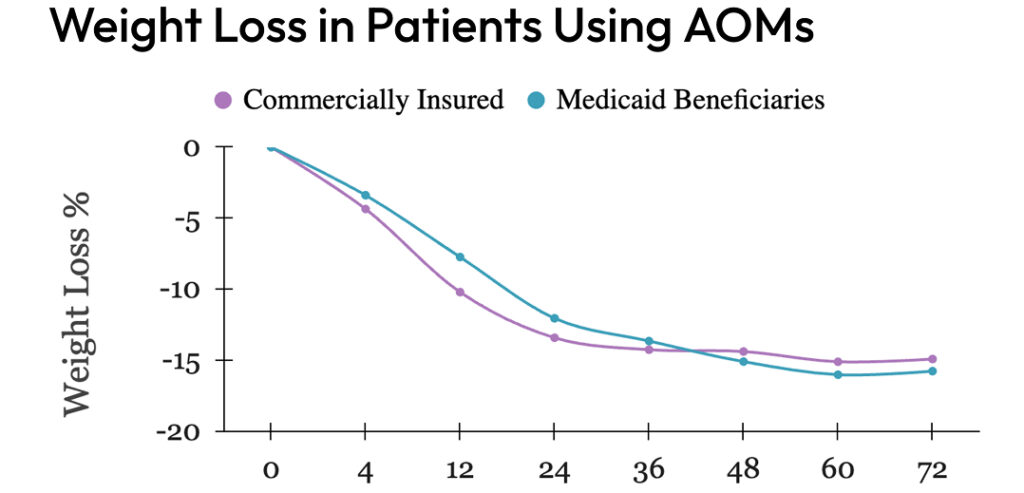
With AOMs: The gap nearly disappeared
This data fuels Enara’s advocacy for broader Medicaid coverage of evidence-based obesity medications.
Clinical takeaway: If you’re managing a Medicaid-heavy population, AOM access isn’t optional—it’s equity in action.
“When I finally got approved for the medication, everything changed. It wasn’t just the pounds—it was the blood pressure, the energy, the hope. Before that, I felt like I was doing everything right and still losing.”
Medicaid Enara patient, after starting AOM at month 6
Background
Prior research highlights differences in access to and efficacy of obesity treatments across socioeconomic and racial groups. This study examines weight loss outcomes in an obesity management program, comparing adults with Medicaid insurance to those with commercial insurance, both with and without anti-obesity medications (AOMs).
Methods
A retrospective cohort study was conducted with adults enrolled in an obesity management program. Participants were divided into 12-month and 18-month cohorts. Within each cohort, those with Medicaid insurance were matched with those having commercial insurance using propensity score matching. The matching ratio was 1:2 for the 12-month cohort and 1:4 for the 18-month cohort, based on demographic variables (age, gender, BMI), cardiometabolic laboratory values, and AOM usage. The primary outcome was the percent change in baseline weight at 12 and 18 months.
Results
In the 12-month cohort, Medicaid participants (n=119) lost significantly less weight than those with commercial insurance (n=270): 9.28% vs. 12.63%, p<0.001. In the 18-month cohort, similar trends were observed: Medicaid (n=57) vs. commercial (n=238): 9.81% vs. 13.19%, p=0.02. Among AOM users, weight loss outcomes were similar between Medicaid (n=67) and commercial insurance (n=158) groups in the 12-month (11.72% vs. 13.52%, p=0.14) and 18-month cohorts (15.77%,n=30 vs. 14.87%,n=150, p=0.67). Non-AOM Medicaid participants(n=52) consistently lost less weight than their commercial insurance counterparts(n=112) in the 12-month (6.7% vs. 12.11%, p<0.001) and 18-month cohorts (4.98%,n=27 vs. 12.46%,n=88 p<0.001).
Conclusion
This study highlights significant disparities in weight loss outcomes between Medicaid and commercial insurance participants in an obesity management program, consistent with existing literature on healthcare disparities. Notably, the use of AOMs helps ameliorate these disparities, underscoring their critical role in achieving equitable health outcomes. These findings emphasize the need for policy interventions to enhance access to effective weight-loss medications for Medicaid populations. Addressing these disparities is crucial for improving obesity management and ensuring equitable healthcare for all socioeconomic and racial groups.
Authors: M. Rami Bailony1, Hassan Kafri2 , Patricia Dizon3 ,University of California, San Francisco, CA; University of Damascus, Syria; University of Santo Tomas, Manila